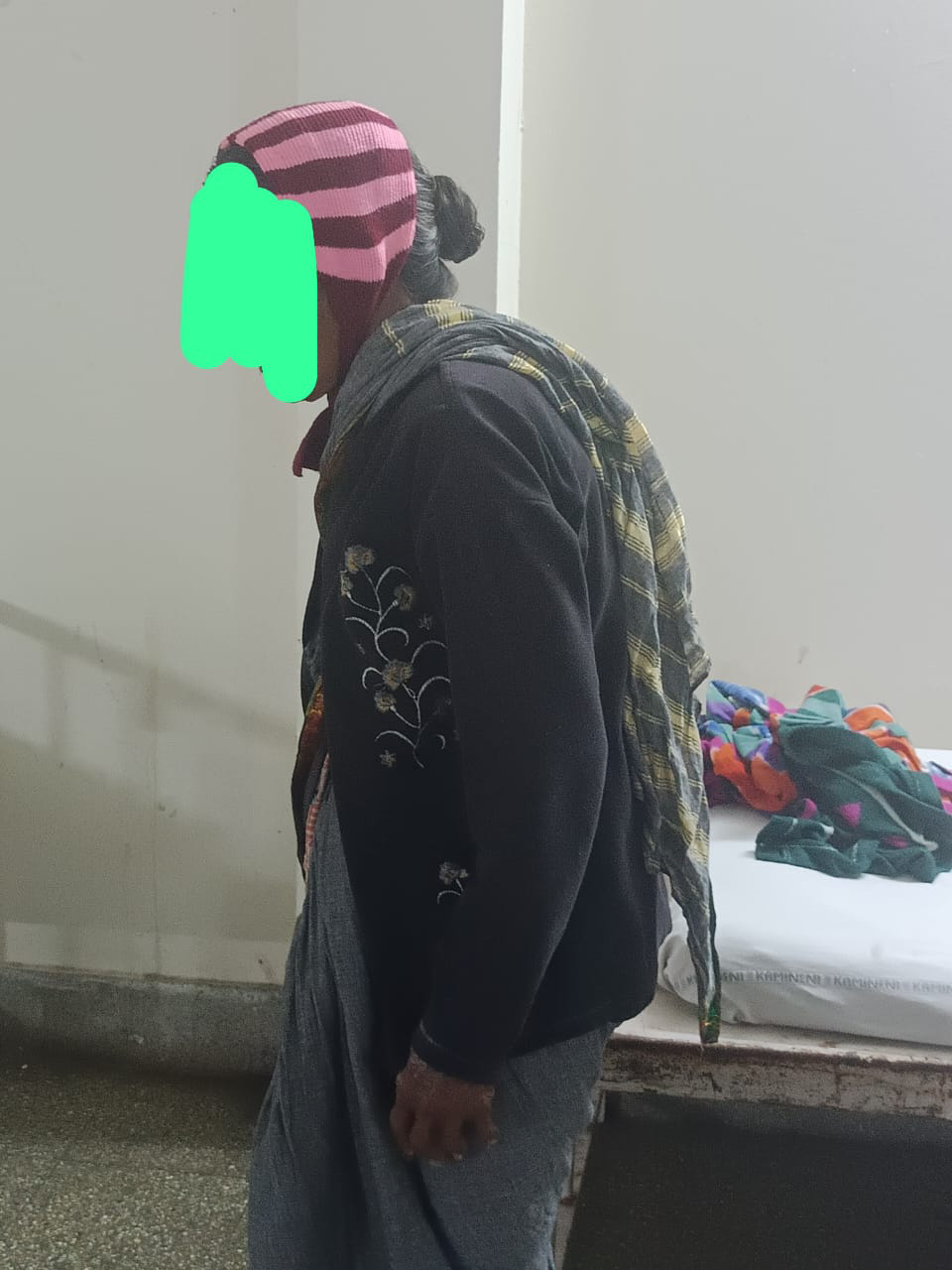
75 yr old female with pedal edema and resting tremors
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
The patient/ attender was informed the purpose of the information being acquired. An informed consent was taken from patient/ attender and there is omission of information that was requested to be omitted.
CONSENT WAS TAKEN FROM BOTH PATIENT AND ATTENDERS
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
The patient/ attender was informed the purpose of the information being acquired. An informed consent was taken from patient/ attender and there is omission of information that was requested to be omitted.
CONSENT WAS TAKEN FROM BOTH PATIENT AND ATTENDERS
A 75 yr old female was brought to opd with chief complaints of
Pedal edema since 1 year
Resting tremors since 1 year
HISTORY OF PRESENT ILLNESS
She was apparently alright 7 years ago when she was diagnosed with hypertension and was started on Tab Amlodipine 5mg + Tab Atenolol 50 mg. She has been on regular medication since then.
1 year back she developed pedal edema extending till the knees, insidious onset, gradually progressive, pitting type.
She also developed involuntary movements of right upper limb at rest which were insidious onset, gradually progressive and no aggrevating and relieving factors, 2 months later she developed involuntary movements of left upper limb also.This has been progressing and she is unable to do her regular activities.
Past history
No history of diabetes, asthma, epilepsy,CAD ,CVA.
Personal history
Appetite : reduced
Diet :mixed
Addictions: stopped talking alcohol since 3 months
Tobacco chewing stopped 3 months ago
General physical examination:
Patient is conscious, cooperative, Oriented to Time place and person.
Built: thin
Posture
Gait
Tremors
Vitals:
Pulse 80bpm
Blood pressure 110/70mmHg
Respiration 17cpm
Temperature. 98.7F
Pallor present
Pedal edema present

No Icterus Cyanosis Clubbing and lymphadenolathy
Systemic examination.:
CNS examination:
Higher mental function examination
Intact
speech : slow
Behavior : normal
Memory : intact
CRANIAL NERVE EXAMINATION:
Normal
MOTOR EXAMINATION: Right Left
UL LL UL LL
BULK N N N N
TONE Rigidity N N N
Cogwheel type of rigidity in right upper limb
POWER 5/5 5/5 5/5 5/5
SUPERFICIAL REFLEXES:
CORNEAL. present present
CONJUNCTIVAL present present
PLANTAR N N
DEEP TENDON REFLEXES:
BICEPS 2+. 2+
TRICEPS 2+. 2+
SUPINATOR. 2+. 2+
KNEE 2+. 2+
ANKLE 2+. 2+
SENSORY EXAMINATION:
Normal
CEREBELLAR EXAMINATION
Normal
SIGNS OF MENINGEAL IRRITATION: absent
Cerebellar functions
Normal
RESPIRATORY SYSTEM:
-Bilateral air entry present
-Normal vesicular breath sounds heard ,
CARDIO VASCULAR EXAMINATION
-S1 S2 heard
-No murmurs
Provisional diagnosis
Parkinson's disease and pedal edema secondary to usage of Amlodipine.
Investigations






Discussion
Role of long term usage of CCBS and pedal edema
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6383103/
This study concludes that a significant number of the patient under antihypertensive medication developed dose-dependent pedal edema. Vasodilatory edema in this study was associated with the presence of other comorbidities, amlodipine dose, and duration, while age, gender, type of amlodipine, and concurrent use of ACEIs/ARBs were not associated. With comorbidities, longer duration, and a higher dose of amlodipine, likelihood of pedal edema goes up. This article adds the prevalence of pedal edema in hypertensive individuals under amlodipine and relation between pedal edema and other variables


Comments
Post a Comment