65 year old female with acute CVA
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Patient and his/her attenders have been informed and their consent has been taken.
65 yr old female was brought to the casualty with complaints of
Difficulty in moving upper limbs and lower limbs since 3 days
Inability to speak since 3 days
Fever since 3 days
HOPI
Patient was apparently alright 2 years back when she was diagnosed with hypertension and is on medication since then
6 days back she developed weakness in left upper and lower limbs which was sudden in onset , gradually progressed and is completely unable to move since 3 days
She also has fever since 3 days
No H/O Head Trauma (for haemorrhagic stroke)
No H/O Epilepsy
No H/O projectile vomiting, headache or blurring of vision
No H/O recent surgeries (for embolic stroke)
Past History: -
No H/O similar complaints in the past
She is a hypertensive and is on medication since 2 years
-No H/O DM, TB, Hypo/Hyperthyroidism/ Epilepsy/ Asthma/COPD/ CAD/ Blood transfusions/ Connective tissue disorders (stroke in young)
-No H/O Major hospitalizations
-No H/O major surgeries
PERSONAL HISTORY
➤Occupation: Homemaker
➤Patient is married .
➤Patient takes mixed diet and has a decreased appetite.
➤Bowel and bladder movements are normal
➤No known allergies .
➤No addictions
General examination
Pt is drowsy, non responsive
BP 150/80 mmHg
PR 85bpm
TEMPERATURE 102 degree F
Grbs 86 mg/dl
Pallor+
No icterus, cyanosis, clubbing,lymphadenopathy, pedal edema
Systemic Examination:
CVS‐ S1 S2 heard, no murmurs
RS‐ Normal vesicular breath sounds hears
P/A - No tenderness, no palpable mass
CNS
HIGHER MENTAL FUNCTIONS:
DROWSY, NON RESPONSIVE
MMSE couldn't be assessed
speech : nil
Behavior : couldn't be assessed
Memory : couldn't be assessed
Intelligence : couldn't be assessed
Lobar Functions : couldn't be assessed
CRANIAL NERVE EXAMINATION:
3rd,4th,6th : pupillary reflexes present.
No Nystagmus
MOTOR EXAMINATION: Right Left
UL LL UL LL
BULK N N N N
TONE hyper hyper N N
POWER couldn't be assessed
SUPERFICIAL REFLEXES:
CORNEAL. present present
CONJUNCTIVAL present present
PLANTAR flexor mute
DEEP TENDON REFLEXES:
BICEPS 2+. 1+
TRICEPS 2+. 1+
SUPINATOR. 2+. 1+
KNEE 2+. 1+
ANKLE 2+. 1+
SENSORY EXAMINATION:
couldn't be assessed
CEREBELLAR EXAMINATION
couldn't be assessed
SIGNS OF MENINGEAL IRRITATION: absent
GAIT couldn't be assessed
Cerebellar functions
Couldn't be assessed
Provisional diagnosis
Rt CVA with left hemiplegia with global aphasia
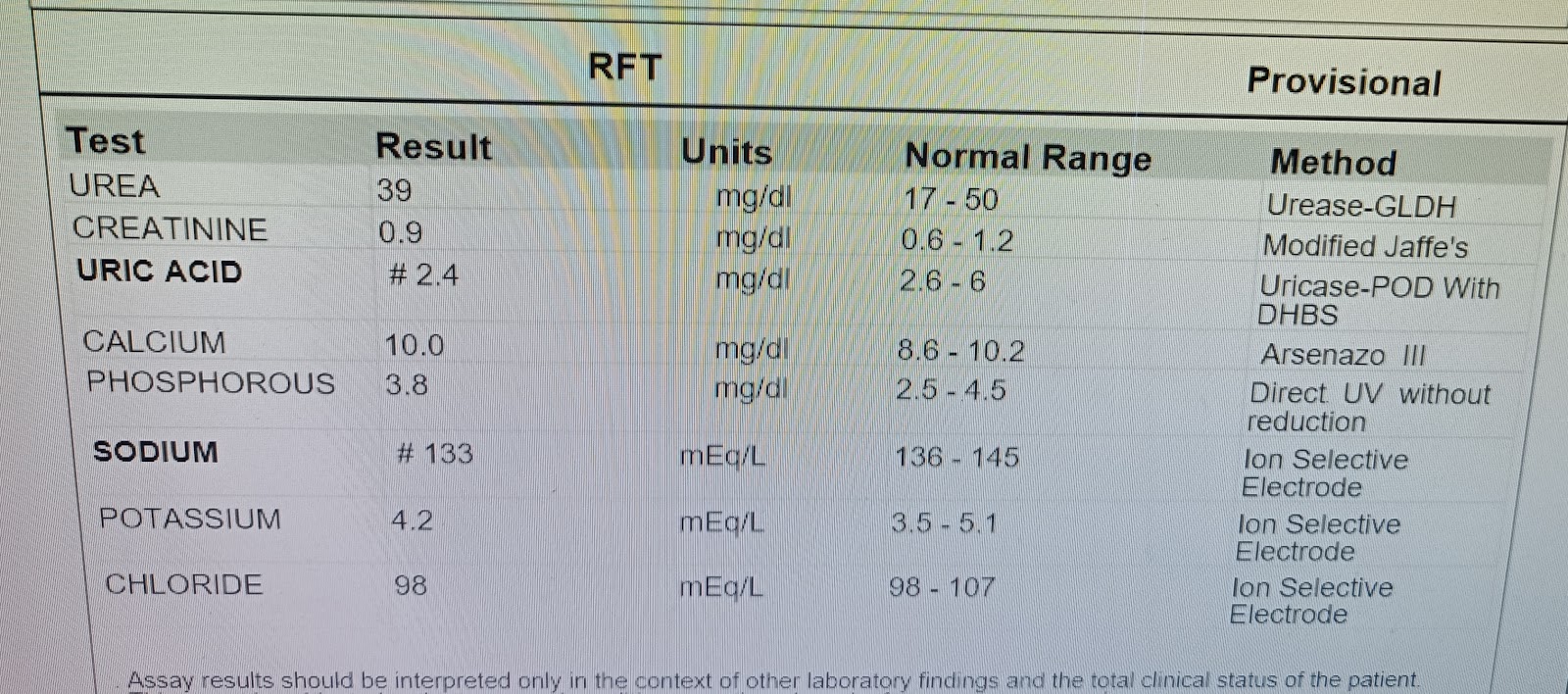
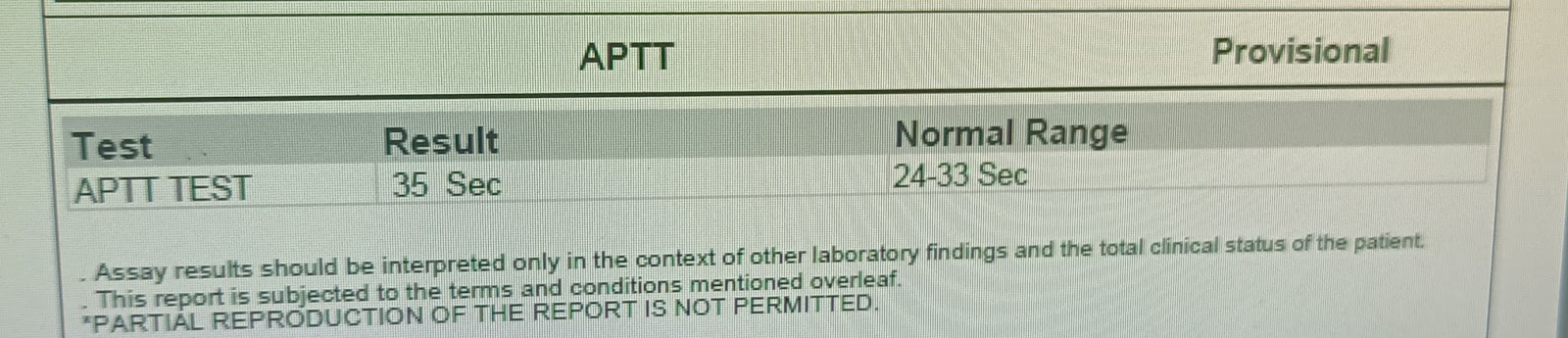
Investigations



Chest x ray







DIAGNOSIS
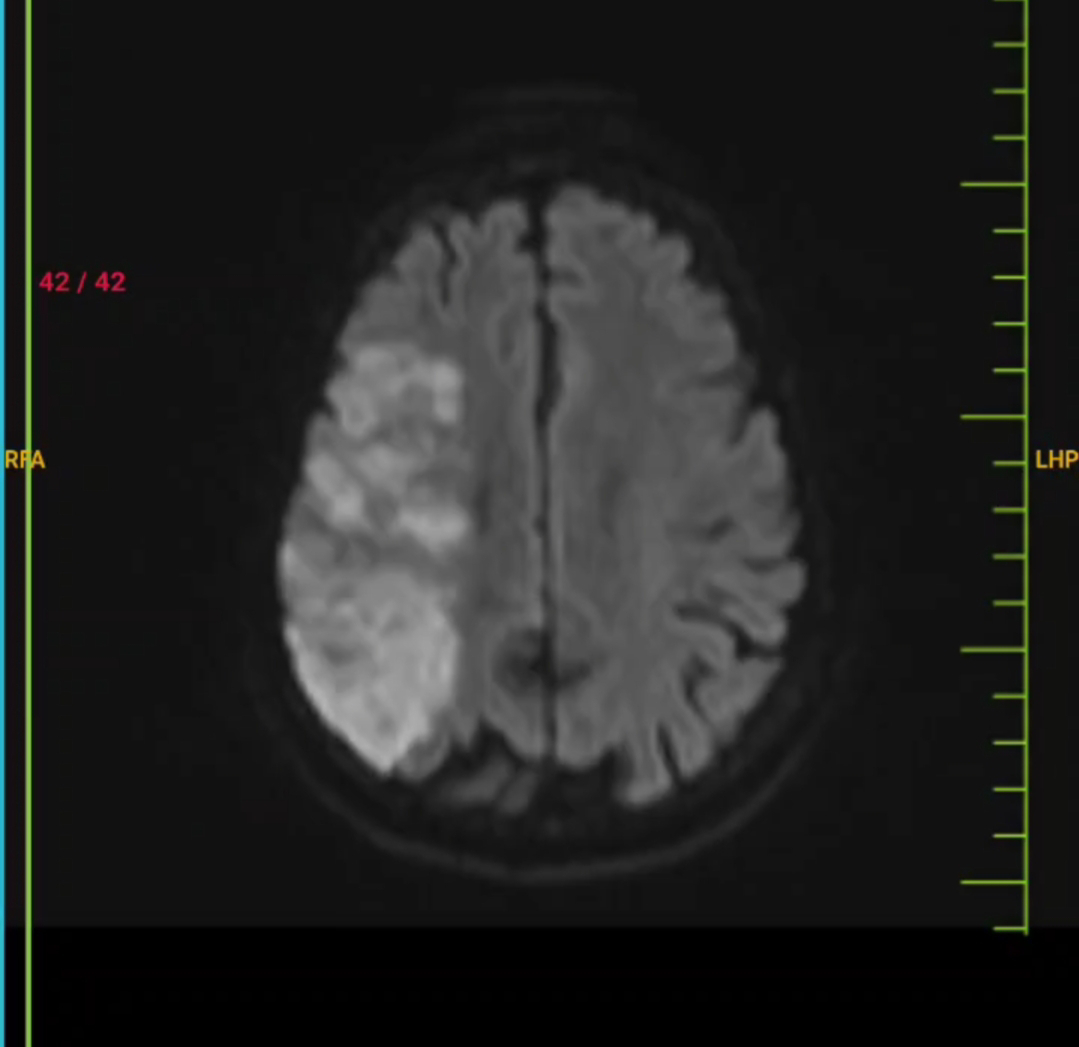
Right sided CerebroVascular Accident with left sided Hemiplegia with involvement of area supplied by middle cerebral artery due to embolism .
Plan of management
1) Ryle 's tube
2) IV FLUIDS
3) Tab ECOSPRIN 150 MG RT STAT
F/B TAB ECOSPRIN 75 mg RT OD
4)Tab ROSUVASTATIN 40 MG RT STAT
F/B TAB ROSUVASTATIN 20 MG RT OD
5) TAB CLOPIDOGREL 150 Mg RT STAT
F/B TAB CLOPIDOGREL 75 mg RT OD


Comments
Post a Comment