ASSESSMENT/CLINICAL PROBLEM SOLVING
This blog is my analysis to a case, as part of CLINICAL PROBLEM SOLVING
I would like to give the analysis of the following blog made by Dr Rashmitha ma'am .
https://potlapallirashmitha.blogspot.com/2021/12/multiple-myeloma.html
I have analysed and interpreted the case into the following headings:
1) Analysis from history, examination, investigations - to rule out the differentials and confirm the diagnosis
2) Understanding the etiopathogenesis of the disease and treatment options
3) Prioritising the problems of the patient and figuring out the best possible options
( with the help of evidence based clinical trial outcomes)
MY ANALYSIS:
PROBLEMS OF THE PATIENT:
COMPLAINTS :
* chief complaints of fever (on and off),
loss of appetite, headache, body pains
*in chronological order :
generalized weakness since 2 months,
cough since 2 weeks
vomitings and pain abdomen since 2 days.
INFORMATION FROM PAST HISTORY
similar complaints 1.5 years
(fever and generalised weakness after which he was diagosed with Anemia and 2 units on PRBCs were transfused)
ANALYSIS FROM PERSONAL HISTORY:
Decreased Appetite
Alcoholic+
Smoking+
ANALYSIS BASED ON EXAMINATION:
Pallor from general examination
NORMAL VITALS
NORMAL findings from CVS,CNS,RESP,PER ABDOMEN EXAMINATION.
ANALYSIS BASED ON INVESTIGATIONS:
From hemogram:
Decreased hemoglobin
Decreased RBC count
Smear : NORMOCYTIC NORMOCHROMIC PICTURE
High RDW - Anisocytosis +
Normal reticulocyte count :THIS RULES OUT HEMOLYSIS AND BLOOD LOSS
POSSIBLE DIFFERENTIALS:
Nutritional anemia(EARLY)
AOCD
Aplastic anemia
Chronic kidney disease
*PCV increased
TLC slightly increased
Normal bleeding and clotting time.
Suggesting no problems in platelets.
*Elevated ESR - suggesting inflammatory changes
*FROM LFT
Elevated total proteins
Decreased serum albumin
Normal A/G ratio
Analysis: Decreased albumin with elevated proteins suggests elevated levels of other proteins - paraproteins /? elevated globulins
Suggesting -? PLASMA CELL DYSCRASIA
*FROM RFT
Increased urea
Increased creatinine
Increased uric acid
Decreased calcium
Increased phosphorus
Slightly decreased sodium
Analysis: renal failure
*Chest X ray:
Right sided effusion
*Normal ECG
*Skull x ray:
shows minor lytic foci
*USG Abdomen -
1. Right mild pleural effusion
2. Right small kidney with normal echogenicity
Analysis:? Right kidney CKD
*HRCT Chest -
1. Moderate to gross right pleural effusion
2. Multilobar consolidations of the right lung, involving upper and middle lobes
3. Passive collapse of basal segments of right lower lobe
*Serum protein electrophoresis:
Decreased albumin
Increased alpha 1
Decreased beta 1
M spike present in gamma region (5.6g/dl)
Analysis:
M band suggests monoclonal band - gammopathy
? Multiple myeloma (myeloma spike)
Other investigations :
Sputum positive for AFB - Pulmonary TB
THYROID PROFILE:
Elevated T3
*Pleural fluid analysis
Pleural Fluid LDH : elevated
Pleural Sugar : elevated
Pleural protein/serum protein : 0.9
- exudate according to LIGHT'S CRITERIA
Pleural Fluid Cytology :
Smear studied showed many neutrophils, occassional lymphocytes against a granular eosinophilic proteinaceous background. No atypical cells seen.
Features of pleural fluid cytology suggestive of Acute Inflammation.
BONE MARROW BIOPSY
which is the investigation of choice for multiple myeloma diagnosis
-Cellularity - Hypercellular M : E ratio = 2:1
-Erythropoiesis -Erythropoiesis suppressed with Normoblastic proliferation. Few megaloblasts are seen.
-Myelopoiesis - Mild myelosuppression seen with orderly maturation
-Megakaryopoiesis - Normal with few hypolobated forms seen
-Lymphocytes and Plasma cells -
Lymphocytes - Normal to increased in number
Plasma cells - Plasmacytosis with approximately 30% mature plasma cells

seen showing abundant basophilic cytoplasm, eccentric nucleus with characteristic cart wheel chromatin perinuclear hoff binucleate forms, mott cells with russell bodies and occassional plasmablasts seen.
Iron stain - Grade 2 (Normal iron stores) - rules out nutritional cause of anemia
Impression - Mild suppression of myeloid and erythroid series.
>30%plasma cells : Indicative of plasma cells dyscrasias.

( Source :Harrison's principles of internal medicine)
So from history and investigations we have come to the diagnosis of MULTIPLE MYELOMA.
( POINTS IN FAVOUR :
*30% plasmacytosis on bone marrow rules out other plasma cell dyscrasias
*Myeloma defining events in the patient :
-Elevated creatinine
-Anemia )
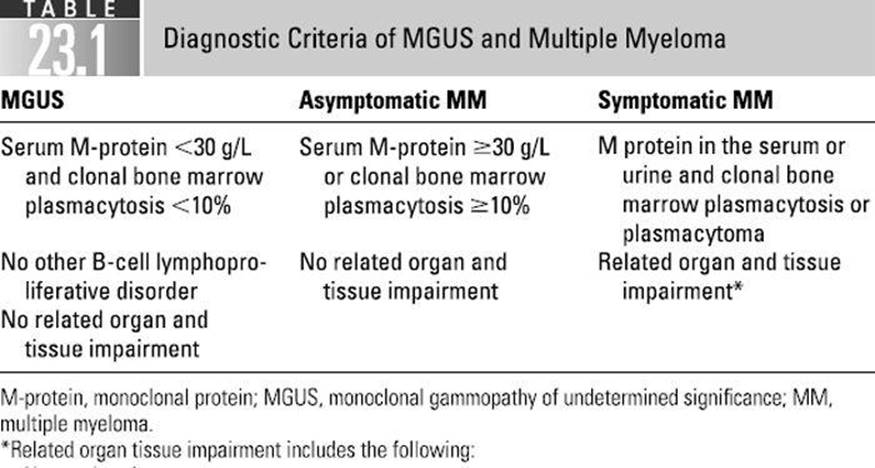
Im adding here the diagnostic criteria for multiple myeloma:


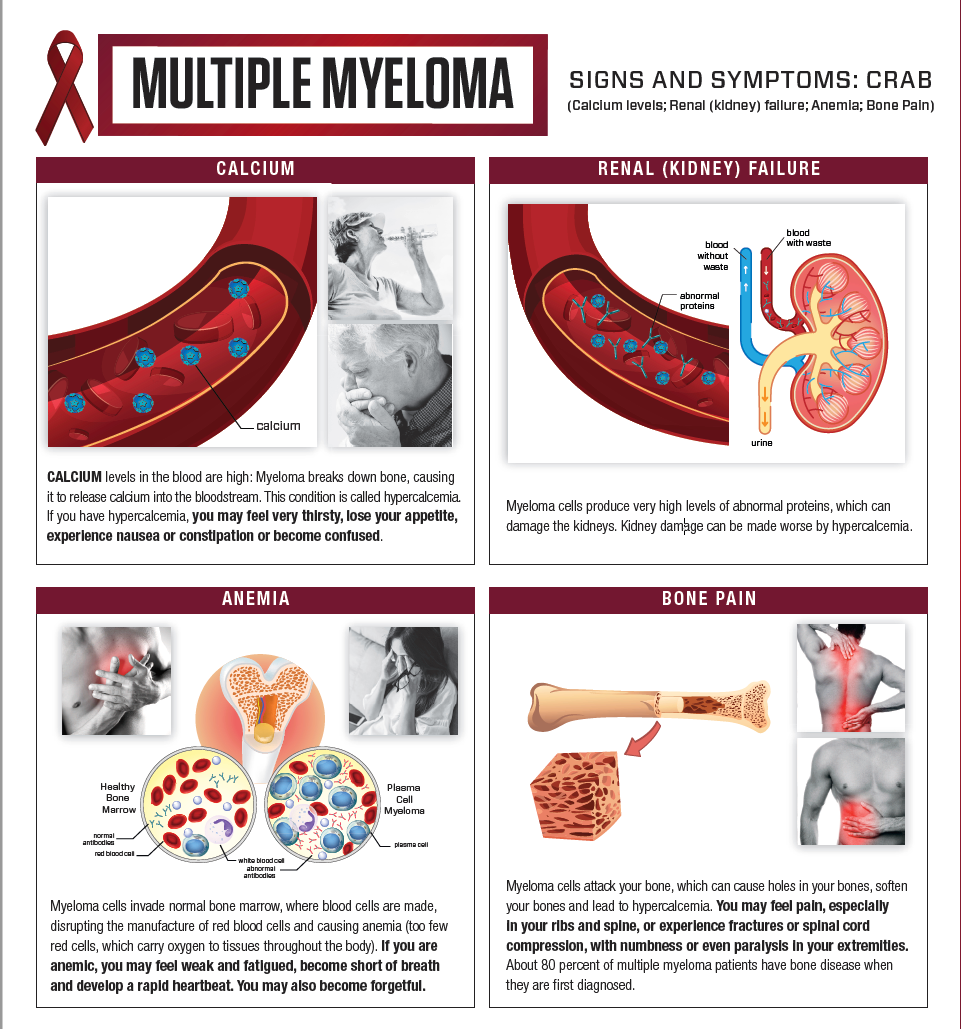
Here, Im adding information about multiple myeloma
MULTIPLE MYELOMA

ETIOLOGICAL FACTORS

CLINICAL SYMPTOMS


marked increase in osteoclastic bone resorption by local factors in the bone marrow
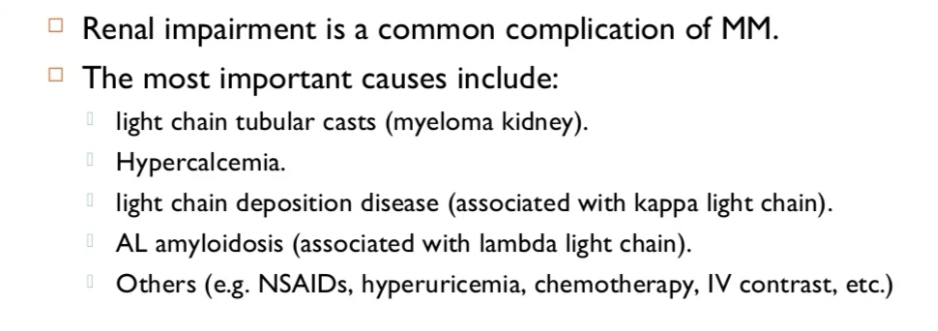
MYELOMA KIDNEY DISEASE
AMYLOIDOSIS : AL Primary AMYLOIDOSIS
INVESTIGATIONS WORKUP :
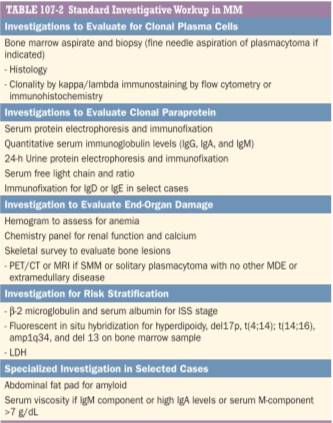
(Source :Harrison's principles of internal medicine)
PRIORITISING THE PROBLEMS AND RELEVANT TREATMENT PLAN:
In the above patient, the main line of treatment here would be to resolve the problem of anemia and renal failure.
Reason for anemia:
Increased plasma cells in the bone marrow affecting erythropoiesis
Reason for RENAL FAILURE :
Could be due to deposition of immunoglobulin or amyloid .
Possible treatment options include :

-Chemotherapy - Targeted therapy


-Radiotherapy
-DEFINITIVE TREATMENT : Autologous stem cell transplant.
CLINICAL EVIDENCE BASED SOLUTIONS:
Here I'm adding links of few clinical trials
Study on chemotherapy trials
https://acsjournals.onlinelibrary.wiley.com/doi/abs/10.1002/1097-0142(197208)30:2%3C382::AID-CNCR2820300213%3E3.0.CO;2-C
https://scholar.google.co.in/scholar?q=chemotherapy+for+multiple+myeloma+clinical+evidence&hl=en&as_sdt=0&as_vis=1&oi=scholart#d=gs_qabs&u=%23p%3D9z1I2sp4cR0J
Study on stem cell therapy
https://pubmed.ncbi.nlm.nih.gov/9787148/
Clinical trial about bone marrow transplanted patients:
https://clinicaltrials.gov/ct2/show/NCT00177047
Other treatment options in acute stage :
Symptomatic treatment

evidence on role of plamsa exchange :
https://pubmed.ncbi.nlm.nih.gov/23589951/
My views on treatment of MULTIPLE MYELOMA:
Early diagnosis of multiple myeloma and starting chemotherapy is generally the opted treatment.
But once end organ damage has occurred, it cannot be reversed. Like the renal damage if once occured we need replacement therapy (dialysis) or any other organ damage like cardiac problem needs organ transplant.
Here, I would like to add my experience of a similar case
http://manisharanga132.blogspot.com/2022/01/56yr-old-female-with-sob-diagnosed-with.html
References:
1)Robbins pathologic basis of disease
2) Harrison's principles of internal medicine
3) Wikipedia


Comments
Post a Comment