This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
The patient is a 46 year old woman , resident of nalgonda,with history of autoimmune disease,
CHIEF COMPLAINTS:
She was brought with complaints of 2 episodes of involuntary movements of upper and lower limbs and hemoptysis in the morning.
HISTORY OF PRESENT ILLNESS :
She developed sudden onset movements of both upper and lower limbs at 5am in the morning which lasted for about 4-5mins , associated with confusion after the episode, without any trigger, aura .
she had an other similar episode while she was brought to the hospital.
She had similar episodes at the hospital.
SHE WAS APPARENTLY ASYMPTOMATIC 13 YEARS AGO,
Then she had low back ache and generalised weakness , for which she visited a local hospital.During the investigations, she was found to be having,?soft tissue overgrowth ,(as said by attenders ,no documentation)and need to get operated, during routine investigations creatinine was elevated, then she was started on conservative management .
(Tab Sodium bicarbonate,Shelcal,Omeprazole,Iron folate)
Since then ,she is on routine followup with hemogram and serum creatinine levels,and her baseline creatinine levels were maintained at 3.2mg/dL.
In june 2022,she developed fever and productive cough associated with SOB for which CT chest was done,showing peripheral ground glass opacities,and septal thickening .
Few days later , she developed swelling of both lower limbs till the level of ankles,which were insidious in onset and gradually progressive.
Then underwent dialysis for the first time through right IJV line,for 4 hours,and was on conservative management.
In September 2022, she developed fluid filled bleb, on one finger and then over all the 10 fingers of hand in 10 days ,some of which ruptured on their own and some were pricked by the patient.
She developed eroding nails and distorted nails , hyperpigmented macules over the face and itching over the palms,and low grade fever associated with loss of apetite and alopecia.
Ulcers over palms , pulp of fingers associated with burning sensation
With autoimmune etiology suspicion, she was investigated further
ANA profile was Positive for
Anti Ro 52
SSA/Ro 60++
SSB/La+.
In view of the persistent low Hb 5-6g/dL,bone marrow aspiration (from right posterior iliac spine)was done for evaluation of anemia.
Then she was started on mycophenolate mofetil 360mg,and later was planned to shift to cyclophosphamide as she is not responding to MMF.( But was not started in view of renal insufficiency).
SHE WAS PUT ON MYCOPHENALATE MOFETIL, HYDROXYCHLOROQUINE , OMNICORTIL .
In November she developed cough with whitish color sputum which is mucoid in consistency and moderate in amount and non blood stained and non foul smelling .
Bilateral swelling of lower limbs till knee,not associated with trauma,and decreased urine output for 2 days,and Shortness of breath( MMRC grade 3),and loss of appetite.
Then ,she was diagnosed as
*?Antisynthetase syndrome
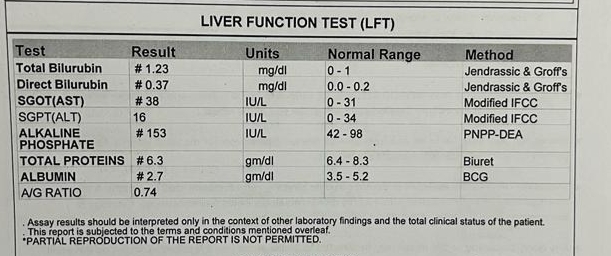
*CLD secondary to autoimmune hepatitis with hypoalbuminemia *
acute exacerbation of ILD
*recurrent anemia
She did not develop any new skin lesions,oral ulcers.
In December,she was taken to another hospital
Due to increase in the SOB with abdominal distension ,
Then she was taken to second session of dialysis.
Her antibody profile was repeated.
Skin biopsy was done
Bronchoalveolar lavage was performed and was found to be having an infective etiology and mucus plugs in the airways.
On ultrasonography,hypoechoic lesions were found in the liver, PET CT was advised and was done.
So they suspected infective etiology probably TUBERCULOSIS,and started her on antitubercular therapy
Tab ISONIAZID 300mg daily
Tab RIFAMPICIN 500 mg OD daily
Tab PYRAZINAMIDE 1500 mg thrice a week
Tab ETHAMBUTOL 1200 mg thrice a week
on 15 th December .( But afb, genexpert are all negative)
CURRENT PRESENTATION
sudden onset movements of upper and lowerlimbs, for 3-4 minutes, associated with bleeding from mouth,with brief period of LOC .
similar episode one at 6:00 am, and then 2 similar episodes after they came here at 8:00am.
At presentation her blood pressure was 170/110 mmhg
Her seizures continued each episode about 2 mins and post ictal confusion was present.
inj lorazepam was given,
later leviteracetam and
when her seizures weren’t controlled then sodium valproate was given
She later then had continuous episodes of seizures lasting for more than 45 minutes .
In view of respiratory distress ( sats 60 ),and uncontrollable recurrent seizures she was sedated with IV MIDAZOLAM and intubated.
Post intubation, she had cardiac arrest ( no central pulses palpable ) 2 cycles of CPR done ROSC was achieved and post CPR monitor showed monomorphic VT and 2 times 200 J of DC shock was given and then it reverted to sinus tachycardia.
I examined her on day 2 at our hospital
GENERAL EXAMINATION
Patient is on sedation.
She has hyperpigmentation on the face, upper limbs
Her nails
Single Bleb on the right hand
VITALS:
Temperature:afebrile
BP 160/110mmhg
Pulse 158bpm
RR 37 cpm
SYSTEMIC EXAMINATION
CVS : S1,S2 heard. No murmurs
RS : Bilateral air entry present
Normal vesicular breath sounds were heard
CNS
Meningeal signs were absent
As the patient is sedated, I didn't elicit Sensory examination, Motor examination.
Pupils: mid dilated , reactive to light
DOLL'S EYE : present
Reflexes:
SUPERFICIAL:
CORNEAL REFLEX present
CONJUNCTIVAL REFLEX present
DEEP TENDON REFLEXES:
Rt. Lt
Biceps: 2+ 2+
Triceps 2+. 2+
Supinator. A. A
Knee. A. A
Ankle A. A
PROVISIONAL DIAGNOSIS:
STATUS EPILEPTICUS, seizures sec to
?autoimmune vasculitis
? Metabolic cause( increased urea)
Investigations
ON DAY 1
MRI diagnosis : POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME.
She was maintained on ACMV MODE of ventilator
On day 9, tracheostomy was done and placed on SIMV mode
Weaning protocol was followed, from acmv shifted to cpap and then a trial of piece was done, but her RR was crossing 45 cpm, so she is currently maintained on cpap mode .
To summarise this is a case of 46 year old female with Chronic kidney disease since 13 years, with AUTOIMMUNE INVOLVEMENT ( ANA positive) -involving Skin, Nails, Lungs, Liver
with current complaints of seizures, due to POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME.
Current complexities in the patient:
Difficulty in weaning off from ventilator
No improvement in the GCS , ( Delayed recovery or due to cerebral insult? )
Severe anemia
Refractory metabolic acidosis
My questions regarding this case:
1) Does the current problem, seizures fit into the autoimmune spectrum ( vasculitis) ?
Is PRES associated with autoimmune diseases?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2861971/
quoting the important lines:
CONCLUSION: A substantial proportion of patients with PRES have underlying autoimmune conditions that may support endothelial dysfunction as a pathophysiologic mechanism. On brain imaging, the location and severity of vasogenic edema were mostly similar for the different clinical subgroups.
(Of 120 patients of PRES, 54 patients with autoimmune disease, 35 (65%) had cerebellar involvement ,a statistically significant increase compared with those without autoimmunity (P=.008). Half of these had mild edema and half had moderate to severe edema. Asymmetry was also seen in half (27 [50%]). Immunosuppressed patients (n=49) also showed a fairly even combination of mild (24 [49%]) and moderate to severe (25 [51%]) edema.)
Other data:
This article has case reports of
various autoimmune disorders, which presented with PRES features.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6346878/#:~:text=Posterior%20reversible%20encephalopathy%20syndrome%20(PRES)%20presents%20with%20cerebral%20vasogenic%20oedema,with%20confusion%20may%20have%20PRES.
2)Was starting on antitubercular prophylactic therapy needed, even after her investigations were negative?
It was based on clinicoradiological diagnosis.
3) How common is anti synthetase syndrome?
Is this case fitting the criteria?
I have read case reports of anti synthetase syndrome patients
https://pubmed.ncbi.nlm.nih.gov/24003680/
This is a case of twenty-eight year-old woman with predominant signs of polymyositis, pulmonary interstitium involvement and with positive anti-Jo1 antibodies was suspected for antisynthetase syndrome. Over the next three months sores and ulcerations have appeared at the fingertips. In the later course of the disease clinical picture of mixed connective tissue disease associated with interstitial lung disease, with a dominant picture of systemic sclerosis have emerged. She was treated with glucocorticoides and immunosuppressive therapy. Patient condition was mostly stable, without significant progression of lung lesions. Early diagnosis and treatment antisynthetase syndrome significantly contributes to more favorable course and outcome of disease. A prerequisite for that are well-defined diagnostic criteria and an appropriate choice of treatment.
Other case reports:
https://pubmed.ncbi.nlm.nih.gov/23062471/
The antisynthetase syndrome (ASS) includes inflammatory myopathy (polymyositis or dermatomyositis), interstitial lung disease (ILD), arthritis, Raynaud's phenomenon, and mechanic's hands, associated with antibodies against aminoacyl-tRNA-synthetases, the most well-recognized being the anti-Jo1 antibody (anti-histidyl-tRNAsynthetase).
4)Will the Autoimmune CNS involvement fit in explanation for delayed recovery of consciousness?
Speaker notes for the presentation of this case
Slide1
Speaker notes :GOOD MORNING everyone
Im Manisha Ranga, student of Final MBBS here to present a interesting case I have seen during my posting, under the title of “ optimising clinical complexities in acute neurological outcomes”
Slide 2
Speaker notes
My patient is 46 yr old female with history of autoimmune disorders, who presented with seizures
Slide 3
SPEAKER NOTES
My patient is a 46 year old woman, homemaker, resident of Nalgonda, who was brought in confused state, with complaints of 2 episodes of involuntary movements of upper and lower limbs since morning.
Slide4
Speaker notes
She was apparently normal when she went to bed the day before, in the morning at 5am , she developed movements involving both upper limbs and lower limbs, each episode lasted for about 4-5 mins , with tongue bite , followed by confusion lasting for few mins.
was not associated with any trigger, aura.
slide 5
slide 6
slide 7
Speaker notes
13 years back,
she had low back ache,which was diagnosed as soft tissue growth
During routine investigations,
she was found to have elevated creatinine .
Since then she was put on conservative management
(Tab Sodium bicarbonate,Shelcal,Omeprazole,Iron folate)
She is on routine followup with hemogram and serum creatinine levels,and her baseline creatinine levels were maintained at 3.2mg/dL.
slide 8
Speaker notes
In june 2022,
She was hospitalized for sob
, fever and cough
She also developed edema few days later,and underwent dialysis for first time
slide 9
Speaker notes
She developed fluid filled blebs on the hands and fingers ,some of which ruptured on their own and some were pricked by the patient.
She developed eroding nails and distorted nails , hyperpigmented macules over the face and itching over the palms,and low grade fever associated with loss of apetite and alopecia.
Ulcers over palms , pulp of fingers associated with burning sensation
Slide 10
Speaker notes
With autoimmune etiology suspicion, she was investigated further
ANA profile was Positive for
Anti Ro 52
SSA/Ro 60++
SSB/La+.
slide 11
Speaker notes
So , she was started on immunosuppressive therapy
Slide 12
In November,
she developed in increased sob, pedal edema, decreased urine output and was admitted in an another hospital.
Slide 13
Speaker notes
They have diagnosed her as antisynthetase syndrome in view of the mechanic hands ,ILD,
cutaneous ulcers and antibody positivity.
Slide 14
Speaker notes
She was admitted again for increased sob and abdominal distension,
in December
Slide 15
Speaker notes
While investigating, on ultrasonography,hypoechoic lesions were found in the liver.
So,PET CT was done.
It showed metabolically active lung consolidation , mediastinal lymph nodes,minimal pleural effusion,splenomegaly, diffusely thickened peritoneum- infective, to rule out KOCH'S
slide 16
Speaker notes
With PET results showing infective etiology probably KOCH'S , she was started on antitubercular therapy.
Slide 17
No past history of seizures
No history of seizures in the family
Current presentation is with 2 episodes of generalized onset seizures
slide 18
SPEAKER NOTES
GENERAL EXAMINATION
The patient was acutely managed for status epilepticus, and as they were refractory,Iv midazolam was started
So she was in a sedated state
Moderately built and moderately nourished
Pallor was present, no icterus ,cyanosis clubbing ,koilonychia,generalized lymphadenopathy,pedal edema
HER VITALS AT ADMISSION
pulse 158bpm
BP 160/110 mmHg
RR 37cpm
and was afebrile
slide 19
Speaker notes
She has HYPERPIGMENTED lesions over face, upper limbs , neck
Slide 20
Speaker notes
She has distorted, eroding nails
Slide 21
Speaker notes
CNS EXAMINATION
After controlling her seizures, with Iv midazolam
when examined
Meningeal signs were absent
Pupils: R to L , mid dilated
DOLLS EYE: present
Corneal and conjunctival are present
Sensory examination is not elicitable
Motor examination
Bulk and tone is normal
Power can't be elicited.
Dtr
Biceps and triceps were 2+
Slide 22
Speaker notes
Provisional diagnosis is STATUS EPILEPTICUS with my differentials being
Sec to autoimmune vasculitis
Sec to metabolic cause ( elevated urea)
Sec to flare up on stoppage of immunosuppressants
slide 23
Speaker notes
MRI revealed hyperintense signal in bilateral subcortical white matter in both cerebral hemispheres , suggesting PRES
Slide 24
To summarise, this is a case of 46 yr old multi system autoimmune involvement.























































Comments
Post a Comment